Amoxicillin remains a first-line treatment for acute otitis media (AOM) in children, typically prescribed for 10 days. Dosage depends on the child’s weight; consult your pediatrician for the correct amount.
Monitor your child closely for improvement. Reduced ear pain and fever within 48-72 hours suggest a positive response. However, continued symptoms after 72 hours warrant a follow-up visit. Persistent fever, severe pain, or worsening symptoms require immediate medical attention.
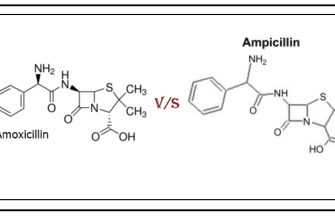
Alternative antibiotics may be considered if your child exhibits an allergy to penicillin or the infection doesn’t respond to amoxicillin. Your doctor will assess the situation and select the most appropriate course of action. Augmentin (amoxicillin-clavulanate) is a common alternative.
Remember: This information is for educational purposes only and does not replace professional medical advice. Always consult your pediatrician for diagnosis and treatment of AOM. Never alter medication dosages without their explicit direction.
- Acute Otitis Media and Amoxicillin
- Factors Influencing Amoxicillin’s Effectiveness
- Alternatives to Amoxicillin
- Monitoring Treatment
- What is Acute Otitis Media (AOM)?
- Amoxicillin: The First-Line Treatment for AOM
- Dosage and Administration of Amoxicillin for AOM
- Potential Side Effects of Amoxicillin in Treating AOM
- Less Common Side Effects
- When Amoxicillin Might Not Be the Best Choice for AOM
- Alternative Treatments and When to Seek Medical Attention for AOM
- Home Remedies: Cautions and Limitations
- When to See a Doctor
- Antibiotic Alternatives and Considerations
Acute Otitis Media and Amoxicillin
Amoxicillin is frequently the first-line treatment for acute otitis media (AOM), a common ear infection in children. However, its effectiveness varies and depends on several factors.
Factors Influencing Amoxicillin’s Effectiveness
- Bacterial Cause: Amoxicillin targets bacteria; viral AOM won’t respond. Accurate diagnosis is crucial.
- Amoxicillin Resistance: Bacterial resistance to amoxicillin is increasing. Local resistance rates influence treatment choice.
- Dosage and Duration: Incorrect dosage or treatment duration reduces efficacy. Follow your doctor’s instructions precisely.
- Patient Compliance: Completing the prescribed course is vital for eradication of the infection.
A high dose of amoxicillin (80-90 mg/kg/day divided into two doses) is often recommended for children with AOM. This is usually given for 10 days. Your doctor will determine the appropriate dose based on your child’s weight and other factors.
Alternatives to Amoxicillin
If amoxicillin fails or isn’t suitable, alternatives include:
- Amoxicillin-clavulanate (Augmentin): This combination combats some amoxicillin-resistant bacteria.
- Cefuroxime: Another antibiotic option effective against many AOM-causing bacteria.
- Azithromycin: A macrolide antibiotic, often used as an alternative when amoxicillin fails.
Always consult a healthcare professional for diagnosis and treatment. They will assess your specific situation and recommend the best course of action. Self-treating AOM is not advised.
Monitoring Treatment
- Symptom Improvement: Note any improvement in symptoms like ear pain, fever, and irritability.
- Follow-up Appointment: Schedule a follow-up appointment to assess treatment response and rule out complications.
- Persistent Symptoms: Contact your doctor immediately if symptoms worsen or don’t improve after a few days of treatment.
Remember, this information is for educational purposes only and does not constitute medical advice. Always seek professional medical guidance.
What is Acute Otitis Media (AOM)?
Acute otitis media (AOM) is a middle ear infection causing sudden onset of ear pain, often accompanied by fever and fluid buildup behind the eardrum. The infection typically involves bacteria or viruses.
Symptoms include earache, fever (often high), irritability, difficulty sleeping, fluid draining from the ear, hearing loss, and sometimes vomiting or diarrhea. In infants, symptoms can be subtle, manifesting as pulling at the ears, crying excessively, or poor feeding.
Diagnosis involves a physical examination of the eardrum using an otoscope. The doctor will look for redness, bulging, or fluid behind the eardrum. Sometimes, further tests might be needed to rule out other conditions.
AOM commonly affects young children due to their relatively horizontal Eustachian tubes, which make drainage more difficult. Treatment often involves antibiotics, such as amoxicillin, to combat bacterial infections. Pain relievers, like acetaminophen or ibuprofen, help manage ear pain and fever. In some cases, myringotomy (a small incision in the eardrum) may be necessary to drain fluid.
Early diagnosis and treatment are vital to prevent complications like hearing loss or spread of infection. Always consult a doctor for suspected AOM.
Amoxicillin: The First-Line Treatment for AOM
For most children with acute otitis media (AOM), amoxicillin is the recommended first-line antibiotic. This is based on extensive research showing its high efficacy against common AOM pathogens like Streptococcus pneumoniae and Haemophilus influenzae.
Typical dosage involves 80-90 mg/kg/day divided into two doses. For instance, a 20 kg child would receive 1600-1800 mg daily, split into two doses of 800-900 mg each. Always consult a medical professional for precise dosing instructions based on the child’s weight and other health factors.
Treatment usually lasts for 10 days. Close monitoring for improvement is vital. If symptoms don’t improve after 48-72 hours, consider contacting your physician. They may adjust the treatment, potentially recommending a different antibiotic or further investigation.
Important Note: Amoxicillin may cause side effects like diarrhea, rash, or vomiting. Report any unusual reactions to your doctor immediately. Amoxicillin is contraindicated in patients with known penicillin allergies. Always discuss treatment options with a healthcare professional before starting any medication.
Alternatives to Amoxicillin: If amoxicillin proves ineffective or if the child has a penicillin allergy, alternative antibiotics such as amoxicillin-clavulanate, cefdinir, or ceftriaxone might be considered. The choice depends on several factors including the child’s age, other medical conditions, and the specific bacteria causing the infection.
Dosage and Administration of Amoxicillin for AOM
Amoxicillin dosage for acute otitis media (AOM) depends on the child’s weight and age. Always follow your doctor’s specific instructions.
Commonly prescribed dosages include:
- Children weighing 20-40 kg: 40 mg/kg/day divided into two doses. For example, a 30 kg child would receive 1200 mg daily, given as 600 mg twice a day.
- Children under 20kg: Dosage will be determined by your doctor based on weight. This is often lower than the 40mg/kg/day.
Amoxicillin is usually administered orally, given with or without food. Ensure the child swallows the medication completely.
- Accurate Measurement: Use a calibrated oral syringe or medication cup for precise measurement of the liquid suspension.
- Complete Course: Finish the entire prescribed course of antibiotics, even if your child feels better before the medication runs out. Stopping early can lead to treatment failure and potential complications.
- Missed Dose: If a dose is missed, administer it as soon as you remember, unless it’s almost time for the next dose. Do not double the dose to make up for a missed one.
- Allergic Reaction: Monitor your child for signs of an allergic reaction, such as rash, hives, swelling, or difficulty breathing. Contact your doctor immediately if an allergic reaction occurs.
- Storage: Store amoxicillin according to the label directions. Liquid suspensions usually need refrigeration.
This information is for guidance only and does not replace professional medical advice. Consult your doctor or pharmacist for personalized recommendations regarding amoxicillin dosage and administration for your child’s AOM.
Potential Side Effects of Amoxicillin in Treating AOM
Amoxicillin, while generally safe and effective, can cause side effects. The most common are diarrhea, nausea, and vomiting. These usually are mild and resolve without treatment. However, if your child experiences severe or persistent vomiting or diarrhea, contact your doctor immediately, as dehydration can be a concern.
Less Common Side Effects
Less frequently, amoxicillin may cause a rash. This rash can be mild, but in rare cases, it might indicate a more serious allergic reaction. A severe allergic reaction is a medical emergency and requires immediate medical attention. Symptoms include difficulty breathing, swelling of the face, lips, or tongue, and hives. If you see any of these, seek immediate medical assistance.
Other less common side effects include changes in bowel movements (constipation), yeast infections (especially in girls), and tooth discoloration (more likely with prolonged use). Your doctor can discuss these possibilities and offer strategies to minimize the risk.
While less frequent than the above, amoxicillin can, in extremely rare instances, affect blood cell counts. Regular blood tests are not typically needed for acute otitis media treatment with amoxicillin, but if your child exhibits unusual fatigue or bruising, consult your physician.
When Amoxicillin Might Not Be the Best Choice for AOM
Amoxicillin remains a first-line treatment for acute otitis media (AOM), but several factors influence its suitability. Consider alternatives if the child has a penicillin allergy. A history of penicillin allergy requires careful evaluation and often necessitates a different antibiotic.
Amoxicillin’s efficacy can be reduced by prior antibiotic use. If the child recently received antibiotics, a different drug may be more effective. Specifically, consider alternative treatment if a recent course of antibiotics failed to resolve the AOM.
Severe AOM symptoms might warrant stronger antibiotics. If the child experiences intense pain, high fever, or significant hearing loss, a broader-spectrum antibiotic, such as amoxicillin-clavulanate, should be considered.
Consider the child’s age. Very young infants may require different antibiotic choices due to potential risks and specific susceptibility to different pathogens. Always consult with a pediatrician.
Finally, local antibiotic resistance patterns influence treatment choices. Your doctor considers local antibiotic resistance data when selecting the most appropriate treatment plan. This means what works well in one area might not be as effective in another.
Alternative Treatments and When to Seek Medical Attention for AOM
For mild AOM symptoms in older children, consider pain relief with acetaminophen or ibuprofen, following dosage instructions carefully. Warm compresses applied to the affected ear may also provide comfort.
Home Remedies: Cautions and Limitations
While these measures can ease discomfort, they don’t treat the underlying infection. Never use home remedies like ear candles; they are unsafe and ineffective. These remedies should be used in conjunction with medical advice and only after a proper diagnosis. Always consult your pediatrician before attempting any alternative therapies.
When to See a Doctor
Seek immediate medical attention if your child exhibits any of the following:
| Symptom | Description |
|---|---|
| Severe ear pain | Pain that doesn’t respond to over-the-counter pain relievers. |
| High fever | Temperature above 102°F (39°C) or persistent fever. |
| Hearing loss | Noticeable difficulty hearing or responding to sounds. |
| Drainage from the ear | Pus or other fluid draining from the ear canal. |
| Balance problems | Dizziness, vertigo, or difficulty with coordination. |
| Facial paralysis | Weakness or drooping on one side of the face. |
Antibiotic Alternatives and Considerations
In some cases, watchful waiting might be an option, particularly for otherwise healthy children with mild symptoms. However, this decision should only be made in consultation with a physician who will monitor the child’s condition carefully. They’ll determine the best course of action based on the individual’s health and the severity of their symptoms.